Evaluation of Environmental Public Health Services
PDF Version (672 Kb, 41 pages)
Table of contents
- List of Acronyms
- List of Tables
- Executive Summary
- Management Response and Action Plan
- 1. Introduction
- 2. EPH Description
- 3. Evaluation Scope and Methodology
- 4. Findings on Relevance
- 5. Findings on Effectiveness
- 6. Findings on Efficiency
- 7. Service Transfer
- 8. Cross-cutting Issue: Climate change
- 9. Cross-cutting Issue: Impact of Covid-19
- 10. Conclusions and Recommendations
- References
- Appendix A: EPH Logic Model and Key Performance Indicators
- Appendix B: Evaluation Questions and Issues
List of Acronyms
- AB
- Alberta
- AT
- Atlantic
- EPH
- Environmental Public Health
- EPHO
- Environmental Public Health Officer
- FNHA
- First Nations Health Authority
- FNIHB
- First Nations and Inuit Health Branch
- ISC
- Indigenous Services Canada
- ISC-RO
- Indigenous Services Canada Regional Operations
- LT-DWA
- Long-term Drinking Water Advisory
- MB
- Manitoba
- O&M
- Operation & Maintenance
- ON
- Ontario
- REHM
- Regional Environmental Health Manager
- SK
- Saskatchewan
- QC
- Quebec
List of tables
Table 1. EPH expenditures in $ millions, by type, 2018-2019 to 2020-2021
Table 3. Public health inspections of permanent food facilities, 2015-2016 to 2020-2021
Table 5. Public health inspections of community care facilities, 2015-2016 to 2020-2021
Table 7. Public facilities inspection rates, 2015-16 to 2020-21.
Executive Summary
This evaluation of Indigenous Services Canada's (ISC's) Environmental Public Health (EPH) Services was conducted as outlined in the ISC Five-Year Evaluation Plan and in accordance with the Treasury Board Policy on Results and the Financial Administration Act. The evaluation was undertaken to provide a neutral, evidence-based assessment of program relevance, effectiveness, and efficiency. It also presents findings concerning climate change, service transfer, Gender-Based Analysis Plus, and impacts of the COVID-19 pandemic on the program to the extent possible.
Background
EPH includes a suite of services that falls under Public Health Promotion and Disease Prevention in ISC's 2023 to 2025 Departmental Results Framework (2023a) and was part of the programs and services brought to Indigenous Services Canada by the First Nations and Inuit Health Branch as a part of departmental transformation in 2017. The objective of EPH services is to identify, assess, mitigate and/or prevent human health risks associated with exposure to hazards and potential risks within the natural and built environments. EPH services are delivered by Environmental Public Health Officers (EPHOs) who are employed by ISC or have been transferred to First Nations communities or Tribal Councils. As of September 2024, 43% of the 144 EPHOs who support communities were transferred. As of December 2024, 311 of 634 First Nations have assumed care and control of their EPH services through health Transfer Agreements.
Evaluation Scope and Methodology
The evaluation covers the period 2015-16 to 2020-21, and was conducted by ISC Evaluation with support from a third-party evaluation firm. The evaluation used a mixed-methods approach that included a review of documents, data and literature; key informant interviews with 15 internal representatives and 7 representatives of transferred services; in-person and remote interviews representatives of 11 communities that receive EPH services from ISC; and, a survey of 50 EPHOs employed by ISC.
Main Findings
Relevance
The evaluation found that EPH services are essential and generally well-aligned with First Nations community needs. Strong relationships between EPHOs and communities support effective delivery, but respondents highlighted increasing demand driven by population growth, infrastructure expansion, and climate challenges; with some also noting gaps in youth-focused education and the integration of Elder knowledge.
Effectiveness
While vital to the health of communities, the effectiveness of EPH services is constrained by resource limitations and systemic barriers. This is evidenced by the fact that key performance targets for inspections of food and community care facilities, as well as other public health infrastructure, were consistently unmet, with inspection rates far below standards set by EPH for itself in the National Framework for the Environmental Public Health Program in First Nations Communities South of 60°. Despite these challenges, EPH did achieve its objective of providing 100% access to trained personnel for drinking water monitoring, reflecting success in targeted areas.
EPH has been operating under these conditions for many years, even preceding the evaluation period. In this context, to maximize effectiveness in terms of preventing adverse health events, EPHOs prioritized their tasks based on inherent risk of activities being carried out at a given location, emergency events such as fires and floods, and community requests.
Beyond internal resource limitations, overall effectiveness of EPH services are limited by the fact that EPH has very little regulatory authority to ensure recommendations for corrective actions are implemented; and, while inspection reports and recommendations for corrective actions can be used by communities to identify needs and to advocate for funding, they do not compel any new funding from ISC or Government of Canada programs to address the underlying issues that were identified.
Efficiency
EPH balances operational efficiency with culturally appropriate service delivery, prioritizing relationship-building with communities. Outdated data management systems hinder the program's ability to analyse data and inform priorities.
Service Transfer
The significant share of transferred EPHOs advances departmental service transfer goals but requires ongoing support, collaboration, and funding. Transferred EPHOs are included in communication and training with ISC EPHOs but it appears that there is no national approach or specific policy in place that defines the expectations placed on the Regional Environmental Health Managers (REHM) in ISC's regional offices with respect to interaction and engagement with transferred EPHOs.
Other Crosscutting Findings
Climate change intensifies demands on EPH services, disproportionately impacting First Nations communities through extreme weather, water safety, disease risks, and long-term effects of evacuations, diverting resources from routine work to emergencies.
While this evaluation did include questions related to how intersectional identities were considered in the design of EPH services (including the youth and elders who are the program's stated focus), evidence collected was not extensive enough to support a comprehensive Gender-Based (Plus) analysis of EPH services.
COVID-19 significantly disrupted EPH services, with community access restrictions and shifting priorities coinciding with a 50% drop in inspection rates. EPHOs took on leadership roles in pandemic response, dedicating 23% of their time to communicable disease control, but 69% reported a detrimental impact on EPH service delivery. A lasting positive effect is increased public health awareness in communities.
Recommendations
- Ensure that REHMs and EPHOs have access to current and easily transferable knowledge and information they can use and share with community leaders to inform about the overall nature of EPH services and the role of an EPHO.
- Describe and document the role of an REHM with respect to the level of interaction, engagement and support provided to transferred EPHOs, with the goal of ensuring that a consistent but flexible approach is implemented within and between regions.
- Identify and implement information management technology that would improve the effectiveness and efficiency of public health data collection, analysis, and use in service planning; and, that would improve the access and use of this data by First Nations.
- Revisit and update if required the National Framework, to ensure that EPH standards, inspection targets, and methods of prioritization are reasonable and comparable to other jurisdictions in Canada, and if necessary, seek additional EPH resources to ensure those confirmed targets can be met.
Management Response and Action Plan
Management Response
Environmental Public Health National Office (EPH Division) welcomes this evaluation report and values the opportunity it presents to further improve Environmental Public Health (EPH) service delivery in on-reserve First Nations. While actions will be taken to address the four recommendations in the report, EPH Division will reflect on its totality to further improve EPH Service delivery more broadly. As with all initiatives, EPH Division will work closely with Regional EPH Managers in considering the evaluation findings and addressing the recommendations.
As the evaluation's findings on effectiveness indicate, EPH Services that are vital to community health have been delivered in the context of resource limitations and systemic barriers for many years. Community population growth and infrastructure expansion, alongside climate change and major industrial development, have been key drivers of the expanding gap between what is required for comprehensive EPH Service delivery and what is available. EPH Division has been meeting this pressure to do more with relatively less by developing and implementing strategies with Regional EPH Managers, while EPH Officers work with community leaders to meet the pressure on the ground. Efforts have included the Environmental Public Health Officer (EPHO) Recruitment and Retention Strategy, which is intended to attract more Indigenous people and women to the career and ultimately contribute to efforts to reduce resource gaps and service constraints; the development of a Hazard Prevention Program and accompanying best practices and guidelines for EPH Officers working in communities; risk-based prioritization of service delivery in accordance with the direction of community leaders; and, advocating for consideration of and investment in upstream measures by other sectors that can prevent future EPH hazards and risks. These initiatives are built and rely on the strong relationships pointed to throughout the evaluation report, and will continue alongside activities to address its recommendations.
The recommendations in this report will build further accountability around and advance initiatives that are already underway by EPH Division.
- EPH services is currently using a published resource to introduce the EPH Officer and their role. However, the language is not necessarily accessible to most audiences and is still labelled as a Health Canada resource. The EPH Division is working with communications to improve this resource.
- Transferred EPHOs are considered part of a broad community of practice by FNIHB and are, for example, invited to training events hosted by ISC that contribute to meeting the Canadian Institute of Public Health Inspectors' continuing professional competencies requirements, and to topic-specific webinars. As another example, all written ISC EPH tools and resources are available to transferred EPH Officers. Formalizing the role of Regional EPH Managers in providing this support will ensure predictability for all concerned.
- Activities in support of developing and posting a request for proposals (RFP) for a new digital solution that will improve and modernize EPH data collection and analysis has been slowly moving through the system. Significant milestones have been met, and it is expected that the RFP will soon be published.
- Comparative analysis of EPH Services and their delivery in other Canadian jurisdictions will be required to fully understand whether the National Framework is consistent with standard practices. It is important to note, however, that due to the location, nature and colonization history of First Nations in Canada, in particular those that are remote, isolated, or frequently experience crises, it will be challenging to draw straightforward comparisons and conclusions. The approach taken will be carefully considered and reported on as part of this response.
The involvement of community representatives in this evaluation was invaluable. Community challenges and priorities are central to getting EPH Service delivery right, and as such are the cornerstones to its ongoing relevance and success in preventing and/or mitigating EPH hazards and minimizing risks.
EPH Division looks forward to the further improvement and advancement that will result from addressing these recommendations.
Action Plan Matrix
Recommendation 1
Ensure that Regional Environmental Public Health Managers and EPHOs have access to current and easily transferable knowledge and information they can use and share with community leaders to inform about the overall nature of EPH services and the role of an EPHO.
- Action 1.1: Update the EPH Services booklet that provides an overview of services and roles of EPHOs
- Action 1.2: Develop a deck to accompany the updated EPH services booklet.
Responsible Manager: (Title/Sector)
Director of EPH Division
Planned Start and Completion Dates
Start date: Q1 24-25
Completion:
- Action 1.1: Q3 25-26
- Action 1.2: Q3 25-26
Action Item Context/Rationale
As of January 2025
- Status: Partially Implemented
- Update/Rationale: communications has been engaged and an initial plain language version has been drafted.
Recommendation 2
Describe and document the role of an REHM with respect to the level of interaction, engagement and support provided to transferred EPHOs, with the goal of ensuring that a consistent but flexible approach is implemented within and between regions.
- Action 2.1: Develop and implement a policy, documented in the EPH services' Quality Management Framework, on how to include transferred EPHOs in the EPH services community of practice, regionally and nationally, designed to be evergreen.
- Action 2.2: Develop a guide for transferred and non-transferred EPHO on how to access EPH resources, including the Quality Management Framework, which will be kept up to date should location of these resources be changed.
Responsible Manager: (Title/Sector)
Director of EPH Division
Planned Start and Completion Dates
Start date: Q1 25-26
Completion:
- Action 2.1: Q3 25-26
- Action 2.2: Q3 25-26
Action Item Context/Rationale
As of January 2025
- Status: Implementation did not commence
Recommendation 3
Identify and implement information management technology that would improve the effectiveness and efficiency of public health data collection, analysis, and use in service planning; and, that would improve the access and use of this data by First Nations.
Action : EPHS initiated an IT enabled Project called the Unified Environmental Public Health Infosystem (UnEPHI) several years ago. The project aims to replace and consolidate several existing legacy systems with a new unified one that meets current IT and Security requirements; leverages current mobile technology to allow in-field data collection; and allows First Nation and others access (based First Nations principles of Ownership, Control, Access and Possession) to the data for analysis, trending and to inform decision making. The UnEPHI Project team has identified the Business Requirements for the new solution and an Options Analysis was completed and endorsed by the Department Architecture Review Board (DARB).
- Action 3.1: Together with Public Service Procurement Canada (PSPC), post an open RFP to solicit bids for the new system.
- Action 3.2: Begin implementation and transition to the new system
- Action 3.3: Project closed out
Responsible Manager: (Title/Sector)
Director of EPH Division
Planned Start and Completion Dates
Start date: Engagement with PSPC began 2023
Completion:
- Action 3.1: Q1 25-26
- Action 3.2: Q2 25-26
- Action 3.3: March 31st, 2028
Above mentioned timelines assume, e.g. that bids come in under the amount, over which Treasury Board Authority would be needed. These and other risks are being tracked and managed as part of the overall management of this IT project.
Action Item Context/Rationale:
As of January 2023
- Status: Partially implemented
- Update/Rationale: The request for proposal was undergoing a final review by PSPC and the EPH Division. It is expected to be posted in Q4 2024/25.
Recommendation 4
Revisit and update if required the National Framework, to ensure that EPH standards, inspection targets, and methods of prioritization are reasonable and comparable to other jurisdictions in Canada, and if necessary, seek additional EPH resources to ensure those confirmed targets can be met.
- Action 4.1: Conduct environmental scan of provincial/ territorial EPH indicators and update EPH services indicators, if and as appropriate
- Action 4.2: Update the National Framework.
- Action 4.3: Update the EPH Work load analysis and associated resource needs
- Action 4.4: If appropriate, seek additional resources to address confirmed targets
Responsible Manager: (Title/Sector)
Director of EPH Division
Planned Start and Completion Dates
Start date: Engagement with PSPC began 2023
Completion:
- Action 4.1: Q3 25-26
- Action 4.2: Q1 26-27
- Action 4.3: Q4 27-28
- Action 4.4: Q4 27-28
Project Close out by March 31st, 2028
Action Item Context/Rationale
As of January 2023
- Status: Implementation did not commence
1. Introduction
This document is the final report for the evaluation of Indigenous Services Canada's (ISC) Environmental Public Health (EPH) services. The evaluation was conducted by ISC Evaluation Branch as outlined in in the ISC Five-Year Evaluation Plan and in accordance with the Treasury Board Policy on Result (2016)s and the Financial Administration Act.
2. EPH Description
2.1 History & Context
EPH includes a suite of services that falls under Public Health Promotion and Disease Prevention in ISC's current Departmental Results FrameworkFootnote 1 and was part of the programs and services brought to Indigenous Services Canada by the First Nations and Inuit Health Branch as a part of departmental transformation in 2017. EPH services are delivered in First Nations communities south of the 60th parallel and are meant to comprise comparable services as those delivered off-reserve by public health authorities under public health legislation.
Program documentation provides a history of EPH service delivery, and how these services were delivered in First Nations communities, it goes back to the early 1900's. Prior to the 1900s, many common infectious diseases were thought to be due to bad air or heredity. Scientific discoveries began to transform popular understandings of the transmission and the prevention of infectious diseases, that Individuals and communities could do something to stop the spread of disease and benefit from early detectionFootnote 2. First delivered by public health nurses, EPH services have evolved along with our understanding of how to prevent injury, disease and death from risks in natural and built environments. In 1961 the Community Health Representative training program of Indian and Northern Health Services was initiated at Norway House, Manitoba. Students learned how to take water samples, build privies, organize garbage collection, choose suitable sites for wells, and to identify causes and possible prevention of some diseases. By 1967, EPH services were delivered by two "sanitarians" employed by the department (for the entire country). They provided some inspection services in First Nations communities, but the bulk of their time was involved with basic training and education in sanitation matters. The release of the Lalonde report in 1974 resulted in a broader approach to public health. It challenged traditional views about health and led to national and international initiatives in knowledge development, health promotion, and health protection.
Today, EPH services are delivered by Environmental Public Health Officers (EPHOs) who are employed by ISC or have been transferred to First Nations communities or Tribal Councils. As of September 2024, 43% of the 144 EPHOs who support communities are transferred. As of December 2024, 311 of 634 First Nations that have assumed care and control of their EPH services through health Transfer Agreements.
EPHOs carry out services in accordance with the National Framework for EPH services in First Nations Communities South of 60°. Services are coordinated regionally by First Nations and Inuit Health Branch (FNIHB) Regional Offices, and supported nationally by the EPH Division. North of 60°, EPHO-delivered services are the responsibility of Territorial Governments.
EPHOs provide environmental public health services in eight core areas: food safety, housing, public buildings and community facilities inspections, drinking water, wastewater, solid waste disposal, communicable disease control, and emergency preparedness and response. Key activities include public education, training, and EPH assessments (e.g., public health inspections, investigations, monitoring and surveillance), infrastructure plan reviews and, the provision of advice and recommendations.
2.2 EPH Objectives and Expected Outcomes
The objective of EPH services is to identify, assess, mitigate and/or prevent human health risks associated with exposure to hazards within the natural and built environments in First Nations communities south of the 60th parallel. Responsibility to mitigate or address the identified risks is with the community, supported by funding programs where available. As indicated in the EPH logic model in Appendix A, the intended immediate, intermediate, and ultimate outcomes of EPH activities are as follows:
- Immediate Outcomes:
- First Nations have access to EPH risk identification services;
- First Nations, Inuit and partners have knowledge of EPH issues, risks, and practices; and,
- First Nations and the federal government have capacity to engage in the investigation of environmental hazards.
- Intermediate Outcomes:
- EPH risks are managed in Indigenous communities.
- Ultimate Outcome:
- Indigenous people and communities are healthier.
2.3 EPH Management, Key Partners and Beneficiaries
The delivery of EPH services supports First Nations communities in identifying and recommending corrective action on potential public health risks that could lead to disease, injury and death.
These services are carried out in First Nations communities south of 60º by EPHOs employed by Indigenous Services Canada, First Nations and Inuit Health Branch or First Nation communities and/or Tribal Councils, in accordance with the National Framework for the EPH services in First Nations Communities South of 60º. Services are coordinated regionally by FNIHB Regional Offices and supported nationally by the EPH Division.
ISC-FNIHB's EPH Division's responsibilities include but are not limited to:
- Supporting Regional EPH activities at the national level;
- Developing national EPH policies and frameworks;
- Updating senior management and central agencies about EPH activities through Departmental Planning Reports, Report on Plans and Priorities, Results-based Management and Accountability Framework (RMAF) reporting and evaluation, and other formal and informal reporting;
- Providing input to Treasury Board submissions and memoranda to Cabinet;
- Analysing data at a national and regional level to support decision-making;
- Developing performance indicators and reporting requirements;
- Providing up-to-date and reliable information about environmental public health issues to Region Offices;
- Identifying environmental public health training gaps and opportunities;
- Liaising with internal and external stakeholders such as national Indigenous organizations and other federal departments and agencies;
- Developing public education materials, including materials for use by EPH Officers;
- Providing technical expertise in environmental areas that may impact public health, such as drinking water quality and treatment, wastewater treatment and disposal, and solid waste disposal;
- Managing direct delivery of the Climate Change and Health Adaptation; First Nations Environmental Contaminants; and Baseline Health and Impact Assessments Programs;
- Delivering health and impact assessment services; and
- Providing analysis services for the EPH services.
ISC-FNIHB Regional Offices responsibilities include but are not limited to:
- Establish and maintain effective working relationships with First Nations communities;
- Providing professional and scientific expertise in the development of public health advisories, recommendations, and the application of mitigation measures;
- Advocating for and promoting compliance with provincial and federal acts, regulations, codes, guidelines and standards by conducting broad-ranging assessments, inspections, surveillance, and evaluations;
- Investigating suspected and confirmed communicable and non-communicable disease incidents and outbreaks, participating in emergency planning (including for human-caused and naturally occurring events);
- Providing expert guidance and professional leadership, in collaboration and cooperation with local, provincial, and federal health authorities;
- Providing professional expertise and guidance, from a public health and an environmental sciences lens, in the development of community emergency response planning, and during response and recovery phases of emergencies;
- Developing and delivering educational materials, workshops, presentations, and formal training across a range of audiences;
- Using and performing calibration on specialized testing equipment to sample/monitor for various chemical, biological, and microbiological components in samples such as air, food, soil, effluent, recreational water, and drinking water;
- Collecting and analyzing data, scientific research and reports, continuously challenging and guiding the measuring and assessments of impacts of mitigation measures from a macro perspective, leading the implementation of prevention and control measures and conducting briefings to senior management and senior community leadership as needed, in collaboration with senior medical, health, and other professionals;
- Liaising with First Nation, federal, provincial, and municipal authorities and private industry using risk communication regarding Environmental Public Health issues;
- Developing annual Regional and Community-level Environmental Public Health Work plans; and
- Working with local health authorities, and provincial departments on cross-jurisdictional public health and environmental public health issues, such as drinking water quality, air quality, and communicable disease issues.
First Nations authoritiesFootnote 3 and communities that receive EPH services from ISC play a central role in EPH programming on-reserve. They work in collaboration with EPHOs to identify environmental public health priorities within their communities and to address environmental public health risks. Their responsibilities include, but are not limited to:
- Engaging and coordinating with Environmental Public Health Services and other stakeholders (e.g., health care workers, ISC-RO, provinces, surrounding municipalities, etc.) to develop, approve, and implement Environmental Public Health community and/or regional work plans;
- Working in partnership with EPHOs, First Nations communities, other health workers, and stakeholders to develop and implement recommendations that relate to environmental public health;
- Providing input from a First Nations perspective when consulted on EPH policies, guidelines, and best practice documents;
- Developing local policies and by-laws to protect and improve the health of the community; and
- Reporting, adhering to Terms and Conditions.
2.4 Program Resources
The following table shows expenditures by type made by the Environmental Public Health subprogram. For the average year shown in the table, EPH expenditures total $44.4 million.
- 53%, or $23.5 million, of average annual expenditures was for ISC personnel including Environmental Public Health Officers and associated O&M.
- 47%, or $20.9 million, of average annual expenditures are transfer or other payments to providers of transferred EPH services.
| Expenditure Type | Fiscal Year | Average | ||||||
|---|---|---|---|---|---|---|---|---|
| 2018-19 | 2019-20 | 2020-21 | ||||||
| $ | % | $ | % | $ | % | $ | % | |
| Personnel (Salaries and benefits) | 16.4 | 39% | 16.1 | 36% | 18.6 | 40% | 17.0 | 38% |
| Operations and Maintenance | 7.2 | 17% | 6.6 | 14% | 5.7 | 12% | 6.5 | 15% |
| Transfer Payments | 17.7 | 42% | 22.6 | 50% | 21.6 | 47% | 20.6 | 46% |
| Other subsidies and payments | 0.4 | 1% | 0.2 | 0% | 0.2 | 0% | 0.3 | 1% |
| Total | 41.7 | 100% | 45.4 | 100% | 46.1 | 100% | 44.4 | 100% |
| Source: Government of Canada, GC Infobase. Expenditures and Planned Spending by Program. | ||||||||
3. Evaluation Scope and Methodology
3.1 Scope and Evaluation Issues
The Evaluation of EPH services covered the traditional subject areas of relevance, effectiveness and efficiency over the period from 2015-16 to 2020-21. The evaluation was carried out from December 2021 to December 2024, with data collection occurring from July 2023 to November 2023. In line with ISC's Five-Year Departmental Evaluation Plan (Indigenous Services Canada 2022a), the evaluation sought to understand progress towards service transferFootnote 5, as well the cross-cutting issues of Gender-Based Analysis Plus, the impact of climate change, and the impact of COVID-19 on the delivery of EPH services.
Most provinces were included in the scope of the evaluation, apart from British Columbia where EPH programming is the responsibility of the First Nations Health Authority. Similarly, the responsibility for EPH programming in the territories has been transferred to territorial governments or First Nations and Inuit control as part of land-claims settlements.
This was a streamlined evaluation focused on the suite of services delivered to First Nations communities by EPHOs. Other components of EPH programming contained in the EPH Programming Performance Information Profile, including activities and outcomes related to the Climate Change and Health Adaptation Program, Health and Impact Assessment services, First Nations Environmental Contaminants Program, Baseline Assessment Program of health and the Environment, and environmental contaminants research from a total diet and total environment perspective (e.g., the First Nations Food Nutrition and Environment Study), are not included in the scope of the evaluation. The remaining components are being considered as part of the annual ISC five-year evaluation planning cycle, and will be incorporated as appropriate into related evaluations.
Appendix B of this report lists the specific questions and issues that guided the evaluation.
3.2 Lines of Evidence
The evaluation was informed by the following lines of evidence:
- Review of documents and data including previous evaluations, management plans, annual reports and other internal documents.
- Review of published literature related to Indigenous worldviews on lands and land management, and their intersection with health and well-being; environmental public health service trends and pressures; as well as other themes related to these services.
- Key informant interviews, including n=15 with ISC-EPH services representatives including national officials and Regional Environmental Health Managers (REHMs), and n=7 representatives of First Nations-led organizations providing transferred services.
- Interviews and community visits with representatives of 11 communities that receive services through EPH, including n=5 in-community interviews in Saskatchewan (SK, n=3) and Ontario (ON, n=2), and n=6 virtual interviews with community representatives located in Manitoba (MB, n=3), Ontario (ON, n=2), and Quebec (QC n=1).
- Survey of n=50 EPHOs employed by Indigenous Services Canada. This represents a 66% completion rate from among the n=76 EPHOs invited to complete the survey.
- To the extent possible, the survey design was informed by previous surveys undertaken in 2011 and 2016 to inform past evaluations, to allow for assessment of changes over time.
3.3 Challenges and Limitations
In line with best practices in evaluation (Patton 2002), the following section details the limits and mitigation strategies of the evaluation to provide readers with a sense of the validity and confidence they can have in its findings:
- EPH services are delivered to a vast number of First Nations communities throughout Canada. While efforts were made to obtain feedback from communities across all regions, not all responded to the invitation or declined to participate.
- Many EPH services are delivered by transferred EPHOs. However, the scope and focus of this evaluation is on services delivered by ISC and therefore is not able to report on the totality of EPH services delivered to all First Nations in Canada. To better understand ISC supports for transferred EPH services, the evaluation team held key informant interviews with representatives of First- Nations-led organizations providing transferred services.
- As the evaluation team, including the consulting team at Ference & Company, could not travel to every community or region, a number of mitigation efforts were deployed. These included the survey and virtual interviews with representatives of First Nations-led organizations. However, in-person interviews and virtual interviews may add a layer of complexity in terms of reading non-verbal cues, which could affect the richness of the data. In each interview regardless of location, the evaluation team sought to protect the privacy of interviewees by confirming consent and outlining how participants' data would be stored and used; and has triangulated evidence from the survey, interviews and program data to mitigate the reliability challenges associated with a small sample of respondents.
- The evaluation team, including the consulting team at Ference & Company, did not include any First Nations members and therefore they may not have fully understood the unique cultural perspectives of First Nations in data collection and analysis.
- Progress towards the ultimate outcome of EPH Services was measured, however it is challenging to attribute a causal relationship between long-term changes and immediate activities. EPH Services continues to work to strengthen its performance measurement strategy to ensure accurate and appropriate measures are in place to report on this progress.
- This evaluation covers the period from 2015-16 to 2020-21. Although appropriate at the time the evaluation was launched in 2021, completion was delayed. As a result, ISC will not have the benefit of learnings on the EPH program covering more recent years. In concert with EPH program officials, ISC Evaluation will consider the risk of the limitation and explore opportunities to enhance knowledge of EPH operations through other related evaluations, such as the upcoming evaluation of Water and Wastewater.
4. Findings on Relevance
Finding 1: EPH services are essential and generally well-aligned with First Nations community needs. Strong relationships between EPHOs and communities support effective delivery, but respondents highlighted increasing demand driven by population growth, infrastructure expansion, and climate challenges; with some also noting gaps in youth-focused education and the integration of Elder knowledge.
4.1 Alignment between EPH services and community needs and priorities
A guiding principle for EPH services is to "work with First Nations communities as active partners" (Health Canada, 2009). As such, EPH services are provided at the request or with the agreement of First Nations authorities. The relationship between EPHOs and the communities they serve tends to be positive and based on mutual respect. This dynamic supports the alignment of service delivery with community need. During several community visits, interviewees described positive professional relationships with EPHOs. Among the n=11 interviewees, n=7 made comments related to the strength of the relationship with the EPHO, or the ways in which they are particularly able to remain attentive to the needs of the community. In some cases, this relationship was the result of a long-standing EPHO and in others it was built through a response to an emergency event. The following is a statement made by a community visit interviewee:
"We work closely with our EHO and he's really supportive. He is always there when we need support, especially when we have a boil water advisory, he provides direction and communicates with Chief and Council, and he provides the reports, recommendation, the letters and all of that." (Community visit interviewee).
Areas of focus for EPHOs and communities comprise of drinking water, inspections of public facilities and housing, food safety, emergency management, communicable disease control, and education and training about EPH risks and mitigation strategies. Among the n=11 community visit interviewees, the following were mentioned as the main activities and services provided by the EPHO to their community: drinking water related activities (n=11); housing inspections (n=8); providing reports, recommendations or advice (n=7); communicable disease related (n=4); animal bite incidents (n=4); support during emergency response (n=4); other facilities inspections (n=3); and food safety training (n=3).
Increased First Nations populations on reserve, infrastructure projects, natural disasters and emergencies and other factors can all increase demand for EPH services according to community visit interviewees and EPHOs. Specifically, among the community visit interviewees (n=7) who discussed operating context, most (n=5) indicated that a growth in population, infrastructure and/or housing units has increased the need for EPH services and a few (n=2) described needs related to information or response to climate/emergency related events. Community visit interviewees were asked if their EPH needs were being met. From among n=11 interviewees, a range of responses were provided, with some providing multiple responses. About half (n=6) indicated that needs are being met, with others (n=6) also indicating that in particular, higher priority concerns and requests for services are acted on quickly by EPHOs; n=5 indicated that they want more frequent visits and more work completed by EPHOs than there appears to be time to do.
The following table shows results to the survey question "To what extent does the current suite of EPH services that you can provide match the needs and priorities of the communities you serve?" Most respondents (76%) indicated either complete or significant alignment. A much smaller number of EPHOs (20%) observed "some alignment".
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| Complete alignment | 0% | 0% | 0% | 40% | 0% | 0% | 8% |
| Significant alignment | 71% | 100% | 75% | 50% | 83% | 50% | 68% |
| Some alignment | 18% | 0% | 25% | 10% | 17% | 50% | 20% |
| No alignment | 0% | 0% | 0% | 0% | 0% | 0% | 0% |
| Do not know | 12% | 0% | 0% | 0% | 0% | 0% | 4% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
4.2 Impacts on Diverse Communities
Evaluations of ISC programs and services aim to address the extent to which they account for diverse, intersectional identities of community members, including the needs of youths and Elders. Although there is evidence that the program was designed with diverse populations in mind, primary data collected in this evaluation was not extensive enough to support a comprehensive Gender-Based (Plus) analysis of EPH services.
To illustrate, the Program Information Profile for EPH highlights its focus on specific populations. It notes, for example, that "when prioritizing inspections and when conducting health risk assessments, the populations that use the building is considered. Those locations where specific populations may be found such as infants/children, breastfeeding women, and elders are considered higher risk and prioritized over low-risk locations."
However, when the question of the extent to which EPH supports diverse and intersectional identities was asked to community visit interviewees and internal EPH interviewees, most had no specific response or noted that services are delivered community-wide, and it is difficult to determine how it accounts for population groups specifically. A few internal interviewees (n=3) noted that that by reducing EPH risks, EPH service delivery protects vulnerable populations including both younger and older community members and those with compromised immune systems.
More could be done to direct education and training about EPH risks to diverse audiences such as youth, according to community visit interviewees. Some (n=4) indicated that there was a need for more education and awareness activities directed at youth and/or delivered in schools by EPHOs, and a few (n=2) indicated that greater incorporation of knowledge held by Elders into EPH activities and risk mitigation. The following are related statements made by community visit interviewees.
"More education. Awareness. Spending time in the schools. Bringing in elders into a forum or just talking to them about and getting their feedback too." (Community visit interviewee).
"Maybe there is a missed opportunity for the EPHO to do something at the school, do something like a youth gathering and talk about some of these issues. Maybe he's never been invited to do it. I don't know." (Community visit interviewee).
5. Findings on Effectiveness
Finding 2: While vital to the health of communities, the effectiveness of EPH services is constrained by resource limitations and systemic barriers. Key performance targets for inspections of food and community care facilities, as well as other public health infrastructure, were consistently unmet, with inspection rates far below standards. Despite these challenges, EPH did achieve its objective of providing 100% access to trained personnel for drinking water monitoring, reflecting success in targeted areas.
5.1 Short-term Performance
During the evaluation period, ISC EPHOs carried out an average of about 4,700 inspections of 3,200 unique public facilities annually. While this represented a significant amount of work, the 3 performance indicators that relate to the immediate intended outcome "First Nations have access to environmental public health risk identification services" were not met due to resource limitations. These limitations are discussed further in section 5.4.
The first measure - permanent food facilities are to be inspected at least once annually - aims to achieve a target of 80% annually. The following table shows that inspection rates for permanent food facilities over the evaluation period ranged between 22% (2020-21) and 56% (2015-2016).
| Inspections | Fiscal Year | |||||
|---|---|---|---|---|---|---|
| 2015-16 | 2016-17 | 2017-18 | 2018-19 | 2019-20 | 2020-21 | |
| Number of permanent food facilities | 2,157 | 2,321 | 2,268 | 2,136 | 2,230 | 2,285 |
| Number of facilities inspected at least once | 1,205 | 1,153 | 1,205 | 1,102 | 1,017 | 510 |
| Annual Inspection Rate | 56% | 50% | 53% | 52% | 46% | 22% |
| Performance Target | 80% | 80% | 80% | 80% | 80% | 80% |
| Source: Environmental Public Health Annual Reports. | ||||||
The second measure - permanent food facilities with critical violations identified - aims to achieve a target of fewer than 75% with an unsatisfactory result within an inspection category. As shown in the following table, the target was achieved in some years (2015-16, 2019-20, 2020-21) and not in others.
| Inspections | Fiscal Year | |||||
|---|---|---|---|---|---|---|
| 2015-16 | 2016-17 | 2017-18 | 2018-19 | 2019-20 | 2020-21Footnote 6 | |
| Number of permanent facilities inspected for risk | 1,193 | 1,153 | 1,403 | 1,102 | 673 | 215 |
| Number of facilities with at least one unsatisfactory result within a category | 854 | 922 | 1,235 | 862 | 501 | 142 |
| % of facilities with at least one unsatisfactory result within a category | 72% | 80% | 88% | 78% | 74% | 66% |
| Performance Target | <75% | <75% | <75% | <75% | <75% | <75% |
| Source: Environmental Public Health Annual Reports. | ||||||
The third performance measure for the immediate intended outcome "First Nations have access to environmental public health risk identification services" is that at least 80% of community care facilities are to be inspected at least once annually. As shown in the following table, the target was not met during the evaluation period with the results ranging between 30% (2020-21) and 59% (2018-2019).
| Inspections | Fiscal Year | |||||
|---|---|---|---|---|---|---|
| 2015-16 | 2016-17 | 2017-18 | 2018-19 | 2019-20 | 2020-21 | |
| Number of community care facilities | 1,249 | 1,134 | 1,214 | 1,119 | 1,076 | 1,211 |
| Number of facilities inspected at least once | 715 | 382 | 696 | 661 | 551 | 363 |
| Annual Inspection Rate | 57% | 34% | 57% | 59% | 51% | 30% |
| Performance Target | 80% | 80% | 80% | 80% | 80% | 80% |
| Source: Environmental Public Health Annual Reports. | ||||||
Importantly, the 80% target for the two inspection rates above is actually less than the standard of 100% set out in the National Framework (2009), highlighting that the inspection rate shortfalls for permanent food facilities and community care facilities are more significant than the tables above suggest. Annual, or more frequent, inspection requirements for these types of facilities are typical in other jurisdictions in CanadaFootnote 7. Given that a guiding principle for EPH services is to "strive for a level of on-reserve environmental public health services that is comparable to that available off-reserve and consistent from Region to Region" (Health Canada, 2009), there appears to be continued need for improved inspection rates and targets.
Also of note is the sharp decline in the two inspection rates that occurred in 2020-21, which will be discussed in a later section dedicated to the impacts on EPH of the COVID-19 pandemic.
Moving to the second immediate intended outcome: "First Nations, Inuit and partners have knowledge of potential EPH hazards, risks, and mitigation practices". The target is that 100% of communities have access to trained Community Based-Water Monitors or EPHOs to monitor drinking water quality. This target has been has met and maintained over the evaluation period. All (100%) communities had ongoing access to trained Community-Based Water Monitors or EPHOs to monitor drinking waterFootnote 8.
5.2 Achievement of intermediate and ultimate results
For the intermediate intended outcome: "EPH risks are managed in Indigenous communities" EPH has met but not maintained the related performance target. According to the performance targets, public water systems in First Nations communities are to be monitored for bacteria at a rate of 82% of the recommended number of sampling weeks. As shown in the following table, the target was achieved in 2017-18 (85%) and 2019-20 (83%). The COVID-19 pandemic had a significant impact on both normal, planned, and periodic drinking water activities due to restricted access to communities, which coincided with reduced overall sampling rates in 2020-21 to 70%.
| Inspections | Fiscal Year | |||||
|---|---|---|---|---|---|---|
| 2015-16 | 2016-17 | 2017-18 | 2018-19 | 2019-20 | 2020-21 | |
| Average | 80% | 80% | 85% | 78% | 83% | 70% |
| Source: Indigenous Services Canada. National Drinking Water Program Annual Reports. | ||||||
The ultimate intended outcome of EPH services is that Indigenous people and communities are healthier, which is measured using two indicators. The first is the number of confirmed water/foodborne disease outbreaks Both the baseline (2019-20) and ongoing targets are zero (i.e., no outbreaks), and data are captured by Regional Environmental Health Managers through the Performance Indicator Questionnaire that is provided to the National Office on a yearly basis. As there were no outbreaks during the evaluated period, this target is deemed met, though it is important to acknowledge that factors beyond EPH activities impact the result of this indicator, and that zero incidence does not imply zero risk. The second indicator is the percentage of First Nations and Inuit adults who reported being in excellent or very good health. The baseline rate of 37.8% is derived from the most recent available data from the First Nations Regional Health Survey (2015-16). Progress towards the target (44% by March 2028) is expected to be measured using data from future survey cycles.
5.3 Achievement of EPH Inspection Rate Standards
In addition to the inspection rates that are measured as part of EPH's performance indicators, the National Framework (2009) indicates that a range of public facilities, including health, community care, general, and recreational are to be inspected between 1-4 times per yearFootnote 9.
The following table shows inspection rates by type of public facilities on reserve, ordered by a simple average of yearly inspection rates from high to low. From this data it is evident that inspection standards were generally not met, as no type of facility approached 100% inspection rates in any year of the evaluation period. Coinciding with the immediate performance indicators discussed above, community care and permanent food facilities – already covered in section 5.1 but included here again for comparison – had the highest overall inspection rates relative to other types of facilities.
| Type of facility | % inspected during fiscal year | |||||
|---|---|---|---|---|---|---|
| 2015-16 | 2016-17 | 2017-18 | 2018-19 | 2019-20 | 2020-21 | |
| Community care | 57% | 34% | 57% | 59% | 51% | 30% |
| Permanent food | 56% | 50% | 53% | 52% | 46% | 22% |
| Recreational | 51% | 40% | 68% | 55% | 50% | 14% |
| Solid waste disposal | 49% | 43% | 43% | 38% | 35% | 11% |
| Health | 40% | 38% | 27% | 30% | 27% | 13% |
| Community wastewater systems | 32% | 33% | 28% | 33% | 34% | 12% |
| General | 29% | 26% | 24% | 15% | 18% | 11% |
| Recreational water facility | 22% | 15% | 23% | 32% | 9% | 19% |
| Source: Indigenous Services Canada. Environmental Public Health Annual Reports. | ||||||
EPH has been operating under these conditions for many years, with each EPH annual report during the evaluation period raising the issue of resource constraints and inspection rates that fall below standard. In this context, to maximize effectiveness in terms of preventing adverse health events, EPHOs prioritized their tasks based on inherent risk of activities being carried out at a given location, emergency events such as fires and floods, and community requests. This was highlighted by internal key informants, the majority (75% - 90%) of whom indicated that emergency events and community requests can be prioritized ahead of other work such as routine inspections of lower-risk facilities.
5.4 Delivery Challenges
Workload analysis and other data, such as the inspection rate deficiencies noted above, consistently show that the number of EPHOs is inadequate to fully meet objectives. For example, an internal workload analysis projected a shortfall of 35 EPHOs to meet EPH's 2020-21 targets for inspections, advice and guidance, monitoring, public education, and drinking water activities (Indigenous Services Canada 2021). ISC EPH Activities in First Nations Communities on Reserve Annual Reports make consistent reference to resource constraints throughout the evaluation period, and community representatives in this evaluation indicate that they want more from their EPHOs. For example, from among n=11 community visit interviews, n=5 indicated that they want more frequent visits, and more work completed by their EPHO.
5.4.1 Barriers related to access to EPH risk identification services
Despite the noted constraints, most (54%) EPHOs report that the availability of their services to communities have increased somewhat or significantly over the past 5 years. Others indicate that the availability has stayed the same (32%) or decreased (14%)Footnote 10.
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| Increased significantly | 18% | 0% | 25% | 10% | 0% | 17% | 14% |
| Increased somewhat | 47% | 0% | 38% | 30% | 83% | 17% | 40% |
| Stayed the same | 35% | 33% | 25% | 40% | 17% | 33% | 32% |
| Decreased somewhat | 0% | 33% | 13% | 20% | 0% | 0% | 8% |
| Decreased significantly | 0% | 33% | 0% | 0% | 0% | 33% | 6% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
While the results above suggest that access to services has increased, the annual data discussed above shows the inability of EPH to meet most of its inspection rate targets, and when asked "to what extent do you have the resources available to effectively carry out" activities related to environmental public health assessments, 52% of EPHOs surveyed said "to some extent" and another 10% said "to a limited extent". Just over a third (38%) stated that they had the resources available to effectively carry out EPH activities "to a great extent".
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| To a great extent | 47% | 33% | 38% | 20% | 33% | 50% | 38% |
| To some extent | 47% | 33% | 63% | 60% | 50% | 50% | 52% |
| To a limited extent | 6% | 33% | 0% | 20% | 17% | 0% | 10% |
| Not at all | 0% | 0% | 0% | 0% | 0% | 0% | 0% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
ISC representatives were asked to identify the barriers to communities having greater access to the EPH risk identification services. Beyond barriers related to the overall number of EPHOs, specific items were raised, including access to communities (e.g. winter travel, 'fly-in' communities), the time needed to build trusting relationships between EPHOs and community; COVID-19, natural disasters or emergencies; and the level of community understanding of the EPHO role and skillset.
5.4.2 Barriers related to knowledge of potential EPH hazards, risks, and mitigation practices
EPHOs were also asked the extent to which they have the resources to effectively carry out activities related to public education, awareness and training. Compared to the survey responses regarding EPH assessments discussed above, fewer EPHOs (24%) indicated they are fully able to effectively carry out education, awareness and training activities with current resources, with most responding that they have the required resources "to some extent" (56%), to a limited extent (18%) or not at all (2%).
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| To a great extent | 29% | 0% | 25% | 20% | 17% | 33% | 24% |
| To some extent | 59% | 67% | 50% | 30% | 83% | 67% | 56% |
| To a limited extent | 12% | 33% | 25% | 40% | 0% | 0% | 18% |
| Not at all | 0% | 0% | 0% | 10% | 0% | 0% | 2% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
The following barriers to increasing the level of knowledge in communities about potential EPH hazards, risks, and mitigation practices were noted by key informants:
- turnover of staff and leadership within communities receiving services, as relationships and knowledge about the file needs to be re-established periodically (mentioned by n=4 community visit interviewees and n=4 internal interviewees); and,
- a lack of information management systems and EPHO capacity to fully analyze, utilize and communicate data findings to communities (mentioned by n=2 community visit and n=4 internal interviewees).
Despite the barriers, 62% of surveyed EPHOs indicated that community awareness of environmental public health services increased over the past 5 years (32% said it had stayed the same, 6% said that it decreased). This is similar to the result observed in the 2016 evaluation survey of EPHOs, in which 64% of EPHOs reported that there had been a positive shift in the community members' awareness and knowledge of EPH risks, and higher than the result in 2011 (54%), suggesting that incremental progress is being made. The following is a comment made by a surveyed EPHO about the increase in community awareness of EPH risks:
"The awareness of environmental public health risks has increased significantly over the past 5 years among members of the communities I serve. This increased awareness is primarily due to ongoing community education and outreach efforts, as well as a growing understanding of the importance of environmental health and its impact." (EPHO survey participant).
5.4.3 Barriers related to public health risks being managed in First Nations communities
Finally, respondents were asked about the extent to which they had the resources to effectively carry out activities related to EPH surveillance, including evaluation of data and information, informing development of health advisories or other recommendations, and identifying studies or actions needed to evaluate, mitigate or prevent negative human health effects. Overall, a few (12%) EPHOs responded 'to a great extent', and almost half of respondents (48%) said 'to some extent'. However, many (40%) said to a 'limited extent' or 'not at all'.
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| To a great extent | 12% | 0% | 0% | 10% | 17% | 33% | 12% |
| To some extent | 53% | 33% | 50% | 40% | 50% | 50% | 48% |
| To a limited extent | 29% | 33% | 50% | 30% | 17% | 17% | 30% |
| Not at all | 6% | 33% | 0% | 20% | 17% | 0% | 10% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
The following barriers, which limit the extent to which the EPH services result in public health risks that are managed, were noted by key informants:
- EPH inspection reports and recommendations for corrective actions can be used by communities to identify needs and to advocate for funding, but they do not compel any new funding from ISC or Government of Canada programs to address the underlying issues identified through inspections (mentioned by n=2 community visit interviewees and n=3 internal interviewees); and,
- EPH has very little regulatory authority to ensure recommendations for corrective actions are implemented (mentioned by n=1 community visit interviewees and n=3 internal interviewees).
6. Findings on Efficiency
Finding 3: EPH balances operational efficiency with culturally appropriate service delivery, prioritizing relationship-building with communities. While regional strategies like localized staffing and collaborative planning improve efficiency, outdated technology and data management systems hinder the program's ability to analyse data and inform priorities. Additionally, unresolved systemic issues, such as inadequate infrastructure funding, limit EPH's ability to address recurring public health hazards.
EPHOs and REHMs indicated that although operational efficiencies are important, they must be balanced against culturally appropriate service delivery, which entails time spent building relationships with community members and leadership. The time needed to achieve this increases during times of turnover among staff or leadership. The following quote from a community respondent illustrates this point:
"Our leadership changes every four years, and sometimes they don't understand the scope of people [working as EPHOs] and what they can and can't do, so just some education on what the EPHO is and what they can do would be great." (Community visit interviewee).
FNIHB regions attempt to improve efficiency by positioning staff in geographic regions nearer to the communities they serve, and by developing workplans alongside community leadership to minimize travel inefficiencies. Most (75% - 90%) regional managers indicated that planning is carried out in this manner.
Key informants also noted that outdated technology and data management systems limit EPH's efficiency, and therefore its effectiveness, because data that is collected cannot always be efficiently analyzed and used to inform future priorities. Some ISC employee respondents (n=5) and community visit interviewees (n=4), as well as a few (n=5) EPHO survey participants, noted that they need updated data management systems. The primary concern for these respondents and interviewees is that data management tools like WaterTrax and the Environmental Health Information System (EHIS) are difficult to use, slow, and don't allow for easy data analysis.
The inefficiency of the data management systems is compounded by the lack of available time for EPHOs to conduct analysis of the data. The variety of systems in use are not well-integrated, making it hard for EPHOs to track and share information. This is further complicated by the fact that First Nations leaders have limited access to real-time data, often relying on EPHOs to generate reports manually. A modern, unified system could enable community leaders to access the data directly, improving decision-making and response times. The following statements made by internal key informants and surveyed EPHOs are illustrative:
"Get rid of EHIS. It is very difficult to extract data and very inconvenient to use." (EPHO Survey participant).
"EHIS needs to be replaced with an internet cloud-based system, the idea of still replicating to servers is way outdated." (EPHO Survey participant).
"We have no positions that only work on surveillance - our field EPHOs are far too busy to even to begin to look at surveillance, data, research etc." (EPHO Survey participant).
"Although we do get numerous requests for data, those data requests would be better managed if we had better data collection tools. WaterTrax and EHIS are a big sore point with all of our EPHOs because they're dated and they're not user friendly." (ISC internal interviewee).
Another barrier to overall efficiency is that EPHO public health assessment data is not sufficient on its own to result in systemic change or to increase infrastructure funding in First Nations communities. For example, community visit interviewees noted that homes and other public facilities may be assessed multiple times for the same unresolved health hazards without resolution of critical issues.
7. Service Transfer
Finding 4: Transfer of EPH services to First Nations-led organizations advances departmental goals but requires sufficient ongoing support, collaboration, and funding. Transferred EPHOs are included in communication and training with ISC EPHOs but it appears that there is no national approach or specific policy in place that defines the expectations placed on a REHM with respect to interaction and engagement with transferred EPHOs.
As of September 2024, 43% of the 144 EPHOs who support communities are transferred. As of December 2024, 311 of 634 First Nations that have assumed care and control of their EPH services through health Transfer Agreements. This process began more than 20 years ago. Transferred EPHOs work for Tribal Councils, the BC First Nations Health Authority (FNHA), and other First Nations-led health organizations. As one EPHO serves multiple communities, EPH services are typically transferred to organizations that provide a range of health services to First Nations communities, as opposed to services being transferred directly to the community level. The evaluation included interviews with representatives of transferred services (n=7). In most cases (n=5) the service transfer occurred more than 20 years ago, but some (n=2) occurred in the past 5 years. All (n=7) interviewees indicated that their organizations provide other health services in addition to EPH services.
Representatives of services that had been transferred during the evaluation period described the levels of support they had received from ISC through the transfer process and in setting up their new EPH programs. Successful transfers require training and support from the department during the transition phase. The following is a quote from a transferred EPHO interviewed for the evaluation who received what they felt was adequate support:
"The senior environmental health officer from ISC gave me coaching and mentoring for probably first six months and touching base on all programs that they do, so that we do the same." (Transferred EPHO interviewee).
The other representative of services transferred during the evaluation period described receiving less comprehensive support from ISC:
"I was the first EPHO hired by the Tribal Council to help transfer the program. I spent a month with ISC learning how they do things. I had some support from senior EHO and their manager – but a month is not long enough to do it." (Transferred EPHO interviewee).
REHMs reported that transferred EPHOs are included in communication and training with ISC EPHOs, but some transferred EPHOs (n=2) interviewed for this evaluation have observed decreasing interaction between their program and ISC over time. It is worth noting that the two interviewees were based in the same ISC region and this region had experienced staff turnover in the REHM role throughout the evaluated period; this limits the extent to which the finding can be generalized to other regions. However, it does highlight the fact that there is no national approach or specific policy in place that defines the expectations placed on a REHM with respect to interaction and engagement with transferred EPHOs. The following is a quote from a transferred EPHO speaking about the changes they have observed:
"We're not as engaged with them as we usually are. We had previously been meeting as a region with transferred and non-transferred at least once or twice a year. We haven't met since before COVID. They had been very good at sending us information on programming policies, updates to legislation, and things like that, and that has decreased. So, we've been kind of fending for ourselves a little bit that way." (Transferred EPHO interviewee).
Other challenges related to service transfer were raised by a few (n=3) ISC internal interviewees. Specifically, they noted that existing small-scale (e.g. 1 or 2 EPHOs) transfer agreements do not appear to be sustainable in that it is difficult to maintain services if there is turnover of staff, and the result is the ISC EPHOs need to provide coverage for the communities temporarily without a transferred EPHO.
The limits of small-scale transfers were also highlighted by a few (n=2) transferred EPHOs, who noted that their budgets are not sufficient to establish managerial or specialty expertise capacity within their programs. This contrasts with other transferred EPHOs who work with larger organizations that can contribute additional resources to fund the transferred services leading to more robust and sustainable EPH services.
Community visit interviewees were asked a question which read: "In many cases, EPH services have been transferred from ISC to Indigenous organizations or communities. What is your vision for how EPH services might be delivered in your community in the future?"
Overall, interviewees have had little exposure to how services have been transferred in other instances, limiting their ability to respond to the question. Some (n=3) respondents said they did not feel able to respond to the question given their professional role, suggesting that it would be a community level decision or one to be made by community leadership. Some (n=3) indicated that they think that there would be advantages to having services delivered more locally but that the barrier is financial, and some (n=3) indicated that delivering the services internally fit with their vision or suggested other changes related to increased service or more training for community members.
8. Cross-cutting Issue: Climate change
Finding 5: Climate change intensifies demands on EPH services, disproportionately impacting First Nations communities through extreme weather, water safety, disease risks, and long-term effects of evacuations, diverting resources from routine work to emergencies.
Climate change is likely impacting the delivery and need for EPH services most acutely through extreme weather events and natural disasters such as drought, floods, and wildfire. Research from the National Collaborating Centres for Public Health (2021) discusses the role of climate change in the increasing rate and intensity of natural disasters, as well as how that First Nations peoples are disproportionately affected by natural disasters and emergency evacuations, which can be made worse by existing systemic and structural inequities. Key concerns for long-term evacuations include heightened risks of developing addictions, increased chronic physical health conditions (e.g., asthma and diabetes), increased chronic infectious diseases (e.g., tuberculosis and sexually-transmitted and blood-borne infections), and negative effects on family dynamics (e.g., increases in relationship break-down and intimate-partner violence).
Community evacuations and responding to the damage adverse events cause to homes and facilities can require significant support from EPHOs, reducing the time available to complete routine work and other community priorities. In fact, all REHMs interviewed for the evaluation (n=5) indicated that emergency management and natural disasters impact service delivery.
Key informants were asked "how has or how will climate change impact the delivery and level of effectiveness of environmental public health services?" Of the community visit interviewees who described impacts of climate change (n=7), most (n=4) mentioned water related issues such as lower water levels in the river used for drinking water, excess rainfall or spring runoff causing flooding and erosion. A few (n=2) mentioned availability or safety of traditional foods, increased disease vectors such as ticks and mosquitos, and extreme heat and fires. Internal key informants also highlighted water related issues (n=4), extreme heat and fires (4), and disease vectors (n=3). The following is a statement made by a community visit interviewee.
"When I think about climate change, I think about the water. I think about livelihood, like the hunting and trapping and all of that is all affected by climate change" (Community visit interviewee).
9. Cross-cutting Issue: Impact of Covid-19
Finding 6: COVID-19 significantly disrupted EPH services, coinciding with a 50% reduction in inspection rates.. EPHOs took on leadership roles in pandemic response, dedicating 23% of their time to communicable disease control, but 69% reported a detrimental impact on EPH service delivery. A lasting positive effect is increased public health awareness in communities.
On March 11, 2020, the World Health Organization (WHO) declared the novel coronavirus (COVID-19) outbreak a global pandemic, and Canadian provinces and territories declared states of emergency related to it in late March. The COVID-19 pandemic further impeded the ability of EPHOs to meet inspection targets. From the start of the pandemic, guidance was developed to help in managing and triaging EPH service delivery, while protecting health professionals and those to whom the services were delivered (Indigenous Services Canada 2022b).
There was a marked reduction (approximately 50%) in inspections conducted during the final year of the evaluation period (2020-21) compared to previous years. According to EPH management (Indigenous Services Canada 2022b) this is due in large part to EPHO losing access to communities during the pandemic, facilities not being open due to public health restrictions, and risk prioritization of other EPH services over inspections.
During the COVID-19 pandemic, EPHOs played leadership roles in planning, preparing, and responding to the needs of communities. EPHOs assisted with COVID-19 testing, vaccine delivery/administration, contact tracing and other related activities in First Nations communities. Twenty-three percent of EPHO time in 2020-21 was spent on communicable disease control activities, compared to between 1% and 5% in the previous five- year period (Indigenous Services Canada 2022b).
Among community visit interviewees, n=4 indicated that their EPHO was involved during the pandemic primarily by providing remote education or guidance; n=3 said they were most involved in reopening plans for buildings or helping to establish other community-level processes; and n=2 said that they had little involvement from their EPHO with respect to COVID-19. The following is a quote from a community visit interviewee who had extensive interaction with their EPHO during the pandemic:
"Our schools needed a reopening plan, and he needed to sign off on it; it was a wonderful process, it gave credibility and integrity to the overall public safety of the people; it sounds like one small thing, but it was big. And ripple effects: then the band office, the health centre, the businesses, all needed reopening plans, and he helped get these things back in order in a safe way." (Community visit interviewee).
Despite the work done by EPHOs in responding to the COVID-19 pandemic, the majority (69%) indicated that the pandemic had a detrimental impact on their ability to deliver EPH services. As shown in the following table, the remainder (31%) of EPHOs said that the pandemic had no impact on their ability to deliver EPH services. None felt that the pandemic had had a positive impact on EPH service delivery.
| Province/Territory of Respondent | AB | SK | MB | ON | QC | AT | Total |
|---|---|---|---|---|---|---|---|
| n= | 17 | 3 | 8 | 10 | 6 | 6 | 50 |
| Enabled me to better deliver the full suite of EPH services | 0% | 0% | 0% | 0% | 0% | 0% | 0% |
| No impact on my ability to deliver the full suite of EPH services | 18% | 67% | 57% | 40% | 40% | 0% | 31% |
| Had a detrimental impact on my ability to deliver the full suite of EPH services | 82% | 33% | 43% | 60% | 60% | 100% | 69% |
| Total | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Source: Survey of EPHOs, 2023 | |||||||
Several key informants identified that the COVID 19 pandemic has resulted in more public knowledge about public health in general, and practices like frequent handwashing have continued to be carried out even as the risk has decreased.
10. Conclusions and Recommendations
EPH services are aligned with the environmental public health needs of First Nations communities and are of high importance to the health of communities. Over the evaluated period there have been no major environmental public health outbreaks among First Nations living on reserve. However, while all communities have access to trained professionals to sample drinking water, inspection standards for public facilities (e.g. restaurants, community care facilities) cannot be met with existing resources. Relationships tend to be positive between communities and ISC EPHOs. This allows ISC to be aware of and to direct resources towards community priorities and help risk manage the EPHO shortfall.
Forty-three percent (43%) of EPHOs who support First Nations communities are transferred. This advances departmental goals but requires ongoing support, collaboration, and funding. Transferred EPHOs are included in communication and training with ISC EPHOs, but some transferred EPHOs interviewed for this evaluation have observed decreasing interaction between their program and ISC over time. It is worth noting that the two interviewees were based in the same ISC region; this limits the extent to which the finding can be generalized to other regions, however it does highlight the fact that there is no national approach or specific policy in place that defines the expectations placed on a REHM with respect to interaction and engagement with transferred EPHOs.
Environmental public health (EPH) services face significant challenges with outdated data management systems that hinder its efficiency and effectiveness. Current tools are difficult to use, slow, and don't allow for easy data analysis. The lack of efficient data management, and dedicated time to conduct analysis, means that important trends, like the correlation between housing conditions and health issues, are not being explored.
Some of the key challenges facing the services were also found in the previous evaluation (2010-11 to 2014-15) including high demand for EPH services, the fact that addressing and mitigating EPH risks can often be complex and beyond the scope of EPHOs, and a lack of data to report on longer term impacts (i.e. health of communities and attribution to EPH). A common theme noted across recent health and housing-related evaluations is the barrier to effective service delivery caused by turnover of staff within health and housing positions (Indigenous Services Canada 2022c, 2023b, 2024a, 2024b), and EPHOs and REHMs in this evaluation noted challenges related both to ISC staff turnover as well as turnover of leadership within community. This can create a lack of awareness of the availability and breadth of services. However, other constraints exist such as lack of available funding streams, or awareness of existing funding streams, which could be used by communities to implement EPH recommendations.
Based on the evaluation findings, it is recommended that ISC:
- Ensure that REHMs and EPHOs have access to current and easily transferable knowledge and information they can use and share with community leaders to inform about the overall nature of EPH services and the role of an EPHO. (Supported by Findings #1 and #3)
- Describe and document the role of an REHM with respect to the level of interaction, engagement and support provided to transferred EPHOs, with the goal of ensuring that a consistent but flexible approach is implemented within and between regions. (Supported by Finding #4)
- Identify and implement information management technology that would improve the effectiveness and efficiency of public health data collection, analysis, and use in service planning; and, that would improve the access and use of this data by First Nations. (Supported by Findings #1 and #3)
- Revisit and update if required the National Framework, to ensure that EPH standards, inspection targets, and methods of prioritization are reasonable and comparable to other jurisdictions in Canada, and if necessary, seek additional EPH resources to ensure those confirmed targets can be met. (Supported by Findings #1, #2 and #5)
References
Health Canada. (2009). National framework for the environmental public health program in First Nations communities south of 60 [Internal document].
Indigenous Services Canada. (2021). Environmental public health services workload analysis [Internal document].
Indigenous Services Canada (2022b). Environmental Public Health Program Activities in First Nations Communities on Reserve: 2021/2022 Annual Report [Internal document].
Indigenous Services Canada (2022a). Five Year Departmental Evaluation Plan 2022-2023 to 2026-2027.
Indigenous Services Canada (2022c). Evaluation of the Healthy Living Program.
Indigenous Services Canada. (2023a). Departmental results framework 2023 to 2025.
Indigenous Services Canada (2024a). Evaluation of the Healthy Child Development Program.
Indigenous Services Canada (2024b). Evaluation of the On-Reserve Housing Program.
Patton, Michael Quinn. (2002). Qualitative Research and Evaluation Methods (3rd edition).
Tomes, N. (1998). The gospel of germs: Men, women, and the microbe in American life. Harvard University Press.
Appendix A: EPH Logic Model and Key Performance Indicators
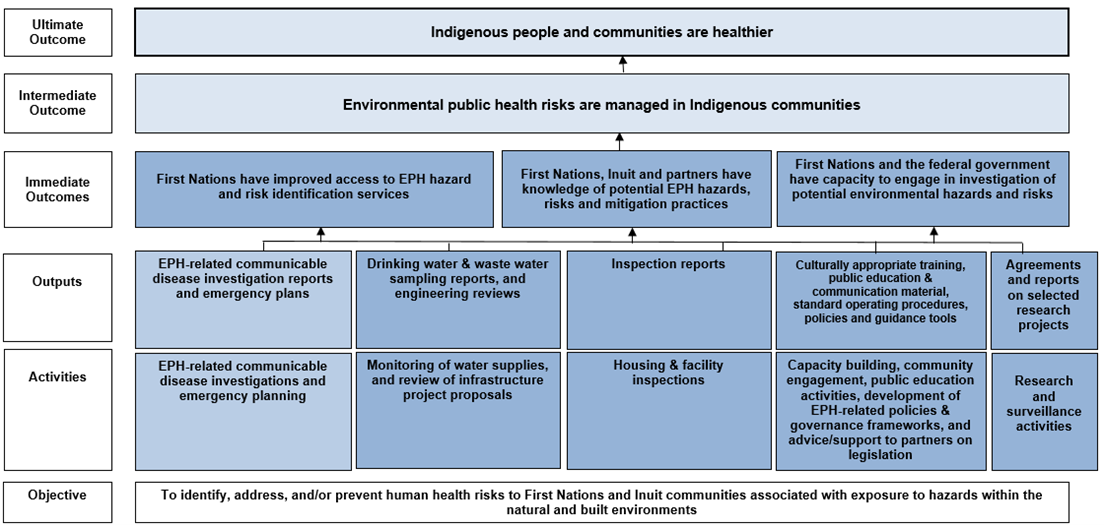
Text alternative for Logic Model for Environmental Public Health Programming
This table represents the logic model for Environmental Public Health (EPH) Services.
The logic model shows that the objective for EPH is "To identify, address, and/or prevent human health risks to First Nations and Inuit communities associated with exposure to hazards within the natural and built environments."
Above this there are five activity streams flowing into five outputs. These outputs together result in three immediate outcomes, one intermediate outcome and one ultimate outcome.
The first activity is EPH-related communicable disease investigations and emergency planning. This produces the output, "EPH-related communicable disease investigation reports and emergency plans".
The second activity is monitoring of water supplies, and review of infrastructure project proposals. This produces the output, "Drinking water and wastewater sampling reports, and engineering reviews".
The third activity is housing and facility inspections, which produces the output "Inspection reports".
The fourth activity is capacity building, community engagement, public education activities, development of EPG-related policies and governance frameworks, and advice/support to partners on legislation. This produces the output "Culturally appropriate training, public education and communication material, standard operating procedures, policies and guidance tools".
The fifth and final activity is research and surveillance activities. This produces the output "Agreements and reports on selected research projects".
All outputs flow into the three immediate outcomes, which are stated as: First Nations have improved access to EPH hazard and risk identification services; First Nations, Inuit and partners have knowledge of potential EPH hazards, risks and mitigation practices; and First Nations and the federal government have capacity to engage in investigation of potential environmental hazards and risks.
The three immediate outcomes flow into the same intermediate and ultimate outcome.
The intermediate outcome is "EPH risks are managed in Indigenous communities". The ultimate outcome is "Indigenous people and communities are healthier."
EPH Output or outcome
Immediate outcomes
First Nations have access to EPH risk identification services
- % of permanent food facilities inspected at least once annually
- % of inspected permanent food facilities with critical violations identified
- % of community care facilities inspected at least once annually
First Nations, Inuit and partners have knowledge of potential EPH hazards, risks, and mitigation practices
- % of communities with access to trained Community Based-Water Monitors or Environmental Public Health Officers (EPHOs) to monitor drinking water quality
Intermediate outcomes
EPH risks are managed in Indigenous communities
- % of the recommended number of sampling weeks that public water systems in First Nations communities were monitored for bacteria
Ultimate outcome
Indigenous people and communities are healthier
- # of confirmed water/foodborne disease outbreaks
- % of First Nations and Inuit adults who reported being in excellent or very good health
Appendix B: Evaluation Questions and Issues
The questions that guided the evaluation are as follows:
Relevance:
- To what extent do these services address continued and emerging needs?
- How has the context within which the services are delivered changed over the evaluation period?
Effectiveness:
- To what extent have expected results been achieved?
- How has service delivery contributed to the achievement of departmental objectives and outcomes?
Efficiency:
- To what extent are the services delivered in an efficient manner?
- How appropriate are the current divisions of roles and responsibilities within and between: national office/EPH Division, Regional offices, delivery partners, and recipients?
Service Transfer
- How might the delivery of EPH services be improved and/or structured to advance service transfer to First Nations partners?
- If service transfer was to happen in your region, what would be necessary to make this feasible; how can the Department better support this transfer?
Cross-Cutting Issues
- How is climate change impacting EPH services and its outcomes/operations?
- How has the design of the EPH services considered: the diverse and intersectional identities of its recipients; and its impacts on youth and elders?
- How has the COVID-19 pandemic effected EPH services (e.g. key challenges, positive or negative effects on planned activities)? What are the main challenges?